前言
腫瘤指數的概念大概就是不太準,主要用於追蹤,但健康檢查還是會做,到底它詳細的敏感度與特異度為和呢?找來找不去,完整的資料實在不多,特別又缺乏明確的資料來源無法判斷品質。以下資料多是一篇篇paper找出來的。其中敏感度與特異度數值若是列為一個範圍,帶表資料來源是多個研究的結果,去一個大概值。若是寫一個明確的數值則是單一個研究的結果。
l 何謂腫瘤指數?
如何能早期診斷出癌症一直是科學家的目標,因此當研究發現腫瘤細胞會釋放特定的物質時,大家都喜出望外。因為似乎只要抽血檢測這些物質,就能發現潛藏的腫瘤。而這些物質就是腫瘤指數。
不過事實往往不盡如人意,大部分的腫瘤指數隊於初期癌症都不準確,也不靈敏。並不是所有腫瘤細胞都會釋放這些物質,或是癌症初期分泌的量太低,跟正常狀況無法區別,等到真正能測得時,癌症往往又太嚴重了。因此腫瘤指數上升不代表一定有癌症,指數正常也不代表一定沒有癌症。處理上可以依風險程度,選擇進一步檢查或追蹤。
l 常用的腫瘤指數
n 癌症胚胎抗原Carcinoembryonic Antigen(CEA)
u 為一種醣蛋白,主要與細胞的相連(Cell adhesion)有關。
u CEA 正常是在胎兒的消化道 (胃及腸道管腔) 中製造,因此成人正常是很少有CEA的存在。
u 主要相關癌症及作為癌症篩檢的敏感度與特異度
|
癌症/閾值
|
癌症期數
|
敏感度
|
特異度
|
|
大腸直腸癌5ng/ml
1
|
整體
|
40-70%
|
90%
|
|
早期(Duke A)
|
20%
|
|
|
|
中期(Duke B,C)
|
30-40%
|
|
|
|
晚期(Duke D)
|
80-90%
|
|
|
|
肺癌2
3.2ng/ml
|
整體
|
70%
|
70%
|
|
早期(TNM I,II)
|
60%
|
|
|
|
晚期(TNM III,IV)
|
80%
|
|
|
|
胰臟癌3
|
整體
|
40%
|
80%
|
|
TNMI4
|
30%
|
|
|
|
TNMII4
|
36%
|
|
|
|
TNMIII4
|
42%
|
|
|
|
TNMIV4
|
51%
|
|
|
|
乳癌5
5 ng/ml
|
整體
|
16%
|
|
|
TNMI
|
6%
|
|
|
|
TNMII
|
11%
|
|
|
|
TNMIII
|
22%
|
|
|
|
TNMIV
|
25%
|
|
|
|
胃癌6
4.7ng/ml
|
整體
|
22.4%
|
|
|
TNMI
|
10%
|
|
|
|
TNMII
|
18%
|
|
|
|
TNMIII
|
20-40%
|
|
|
|
TNMIV
|
80%
|
|
|
|
子宮內膜癌
|
|
|
|
u 其他導致上升的狀況
l 抽菸: 數值可達6ng/ml,因此建議有吸菸者,正常值可設在7至10以上。
l 肝臟疾病,特別是膽道堵塞。
u 整體而言,數值大於10ng/ml一定要進一步檢查。其對早期癌症的敏感度不高,大約都在20%以下。癌症篩檢的種類而言,除了最主要的大腸直腸癌外、肺癌外,另外與胃癌、胰臟癌、乳癌、膽道及膽囊癌都有關。整體而言作為篩檢,CEA有異常,有問題的機會頗大。
n 癌症抗原-125 Carbohydrate Antigen 125(CA-125)
u 相關癌症及作為初期癌症篩檢的敏感度與特異度
|
癌症/閾值
|
癌症期數/閾值
|
敏感度
|
特異度
|
陽性預測率
|
|
卵巢癌7
35ng/ml
|
整體
|
78.7%
|
77.9%
|
3.7%8
|
|
Stage TNM I9
|
46%
|
|
|
|
|
Stage TNM II9
|
92%
|
|
|
u 其他導致上升的狀況
l 月經期:在經期來臨前或當下,會顯著上升。最高甚至到160ng/ml。

10
l 子宮內膜異位
l 懷孕第一期
l 卵巢或子宮炎
l 子宮內膜異位
l 肝炎
l 肝硬化
l 胰臟炎
u CA-125主要用於婦科相關癌症,不過因為女性在停經前,其數值上下變動幅度極大。因此建議對停經前女性,若單看CA-125,其標準值可訂為200ng/ml以上。但也因此停經前用CA-125篩檢卵巢癌的敏感度變得很差,多半需依賴其他指標輔助。整體而言作為篩檢,CA-125有異常,真的有問題的機會不大。
n 癌症抗原19-9 Carbohydrate Antigen (CA-19-9)
u 正常值:37u/ml
u 相關癌症及作為初期癌症篩檢的敏感度與特異度
|
癌症/閾值
|
癌症期數/閾值
|
敏感度
|
特異度
|
|
胰臟癌
<37u ml="" o:p="">
|
整體11
70-80%
70-80%
TNMI4
70%
TNMII4
92%
TNMIII4
75%
TNMIV4
90%
大腸直腸癌<37u ml="" span="">1
整體
40-70%
90%
早期(Duke A)
<10 o:p="">
中期(Duke B,C)
20-40%
晚期(Duke D)
60%
胃癌6
<39ng ml="" o:p="">
整體
12.3%
TNMI
2%
TNMII
8%
TNMIII
10-20%
TNMIV
40%
u 其他導致上升的狀況
l 肝炎。
l 膽結石。
l 膽管阻塞。最高可超過
10000 U/ml。
l 胰臟炎,甚少超過 120 U/ml。
u 人口中約有 7 % 為 Lewis 血型 Le (a-,b-),這些人體內將無法合成 CA 19-9。CA-199主要用於胰臟癌,另外對大腸癌與胃癌也有一定的角色。整體而言作為篩檢,CA-199有異常,真的有問題的機會頗大。
n 癌症抗原153 Carbohydrate Antigen (CA-153)
u 相關癌症及作為初期癌症篩檢的敏感度與特異度
|
癌症/閾值
|
癌症期數/閾值
|
敏感度
|
特異度
|
|
乳癌12
|
整體36ng/ml
|
12%
|
99%
|
|
TNMI 31 ng/ml
|
15%
|
|
|
|
TNMII 31 ng/ml
|
23%
|
|
|
|
TNMIII 31 ng/ml
|
54%
|
|
|
|
TNMIV
|
|
|
u 其他導致上升的狀況
l 懷孕第三期。輕微上升到 50 U/ml 左右。
l 肝硬化。輕微上升到 50 U/ml 左右。
u 由於非乳癌造成CA-153上升的情況很少,因此整體而言,CA-153作為篩檢有異常,真的有問題的機會頗大。
n 癌症抗原72-4 Carbohydrate Antigen (CA72-4)
u 正常值:<6 .7ng="" ml="" o:p="">
u 相關癌症及作為初期癌症篩檢的敏感度與特異度
|
癌症/閾值
|
癌症期數/閾值
|
敏感度
|
特異度
|
|
胃癌13
|
整體
|
16-70%
|
|
|
TNM I
|
12%
|
|
|
|
TNM II
|
15.6%
|
|
|
|
TNM III
|
36.7%
|
|
|
|
TNM IV
|
49.6%
|
|
|
|
大腸癌
|
|
|
|
|
卵巢癌(67.2﹪)
|
|
|
|
|
乳癌(40.5﹪)
|
|
|
|
|
胃癌(44.6﹪),
|
|
|
|
|
胰臟癌(41.7﹪)
|
|
|
|
胃癌stage與CEA,CA199,CA72-4陽性率的關係
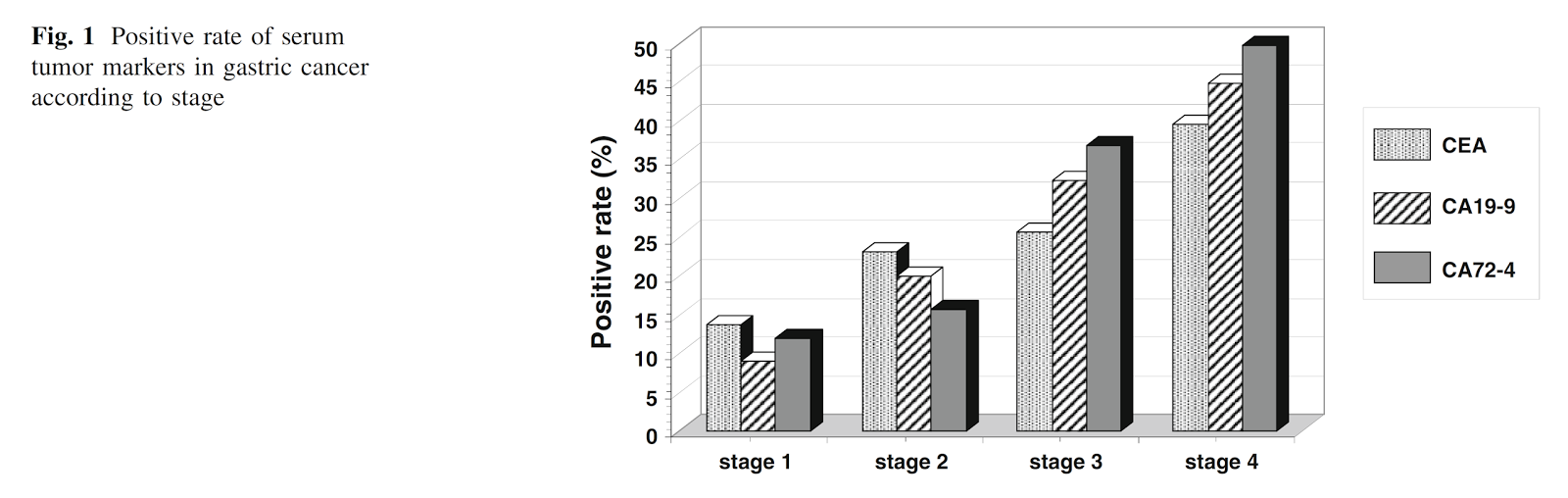
13
u 其他導致上升的狀況
l 胃潰瘍。
u CA72-4是目前對胃癌敏感度最高的腫瘤指數,儘管如此,整體而言也只有40%。
u CA 72-4 有一項很獨特的用途,就是可用來偵測黏液性卵巢癌 (Mucinous ovarian
carcinoma)。因為 CA 125 對大多數的卵巢癌有不錯的偵測效果 (特別是漿液性卵巢癌),唯獨對黏液性卵巢癌的靈敏度較差。因此 CA 72-4 可輔助 CA 125 來提高偵測卵巢癌的靈敏度。
n 前列腺特異性抗原Prostate-specific antigen(PSA)
u 正常值:4ng/ml
u 相關癌症及作為初期癌症篩檢的敏感度與特異度:
l 攝護腺癌:30-70%
|
癌症/閾值
|
癌症期數/閾值
|
敏感度
|
特異度
|
|
攝護腺癌14
|
整體
|
30-70%
|
70-80%
|
|
TNM I
|
|
|
|
|
TNM II
|
|
|
|
|
TNM III
|
|
|
|
|
TNM IV
|
|
|
u 其他導致上升的狀況
l 攝護腺肥大

14
l 攝護腺炎
l 射精或行房亦會使 PSA 上升,一般上升值不超過 1.0 ng/ml。
u 篩檢Screening:
l 此為腫瘤指數中少數被列為可考慮規則篩檢的指數。不過它也是爭議最大的腫瘤指數,因為它十分容易於攝護腺肥大混淆,另外是許多攝護腺癌本身進程很慢,不一定需要治療。
u >25ng/ml很可能已擴散PSA levels of more than 25 ng per mL, the
sensitivity of CT scanning for the detection of positive lymph nodes is only 30
to 35 percent15
u Recommendation for use of PSA
l 美國癌症協會建議男性50歲以上,可以開始與醫生討論”考慮”篩檢PSA(換句話說,也不是一定要)。
l AUA2000
n 攝護腺特異性抗原增加速率PSA velocity
u 建議之標準值<0 .75="" ml="" ng="" span="">年


16
n 年齡別攝護腺特異性抗原標準值Age-Adjusted
PSA
u 建議之標準值
l 40 to 49 years: <2 .5="" ml="" ng="" o:p="">
l 50 to 59 years: <3 .5="" ml="" ng="" o:p="">
l 60 to 69 years: <4 .5="" ml="" ng="" o:p="">
l 70 to 79 years: <6 .5="" ml="" ng="" span="">17

n 甲型胎兒蛋白Alpha-fetoprotein (AFP)
u Alpha-fetoprotein (AFP) 為分子量 70000 daltons 的一種醣蛋白。正常生理情況下,在胚胎卵黃囊、胎兒的肝臟及胎兒的消化道中合成。因此懷孕第四週時,便能在胎兒血清中偵測到 AFP,到第 12 至 16 週時濃度達到最高點,接著開始逐漸下降,直到出生。出生後 1 歲以前,血中 AFP 濃度便降到和正常成人相同。
u 正常值:<20ng ml="" span="">成人),<30ng ml="" span="">一歲前)
u 主要相關癌症與整體靈敏度: 肝癌(41-65%)
|
癌症/閾值
|
癌症期數/閾值
|
敏感度
|
特異度
|
|
肝細胞癌19
<20ng ml="" o:p="">
|
整體36ng/ml
55–60%
88-90%
TNMI
TNMII
TNMIII
TNMIV
u 其他導致上升的狀況:
l 其它癌症的肝轉移:約7%會高,大部分不會高於100ng/ml。
l 懷孕: 可達60ng/ml,約在30週達到高點。
l 肝炎
以下為B肝患者8年內出現AFP上升的狀況

20
l 肝硬化
u 若>500ng/ml,在高危險群個案中,可用來確診有肝細胞癌。
u 由於在有肝炎與肝硬化的病人中,數值本來就會上升,在這類病人身上判斷,需要仰賴其他數據,如超音波。
u 目前少數被列為固定篩檢用的腫瘤指數,但僅用在有慢性肝炎、肝硬化或有肝癌家族史的個案。
1. Hundt S, Haug U, Brenner H. Blood
markers for early detection of colorectal cancer: a systematic review. Cancer epidemiology, biomarkers &
prevention : a publication of the American Association for Cancer Research,
cosponsored by the American Society of Preventive Oncology. Oct
2007;16(10):1935-1953.
2. Okamura K, Takayama
K, Izumi M, Harada T, Furuyama K, Nakanishi Y. Diagnostic value of CEA and
CYFRA 21-1 tumor markers in primary lung cancer. Lung cancer. Apr 2013;80(1):45-49.
3. Yimin Zhang JY,
Hongjuan Li,Yihua Wu,Honghe Zhang,Wenhu Chen. Tumor markers CA19-9 CA242 and
CEA in the diagnosis of pancreatic cancer a meta-analysis. Int J Clin Exp Med. 2015;8(7):11683-11691.
4. Louhimo J, Alfthan
H, Stenman UH, Haglund C. Serum HCG beta and CA 72-4 are stronger prognostic
factors than CEA, CA 19-9 and CA 242 in pancreatic cancer. Oncology. 2004;66(2):126-131.
5. A Re-Evaluation of
Carcinoembryonic Antigen (CEA) as a Serum Marker for Breast Cancer: A
Prospective Longitudinal Study. Clinical
Cancer Research. 2001 7:2357.
6. Zhou Y-C, Zhao H-J,
Shen L-Z. Preoperative Serum CEA and CA19-9 in Gastric Cancer - a Single
Tertiary Hospital Study of 1,075 Cases. Asian
Pacific Journal of Cancer Prevention. 2015;16(7):2685-2691.
7. Dodge JE, Covens AL,
Lacchetti C, et al. Preoperative identification of a suspicious adnexal mass: a
systematic review and meta-analysis. Gynecologic
oncology. Jul 2012;126(1):157-166.
8. Buys SS, Partridge
E, Greene MH, et al. Ovarian cancer screening in the Prostate, Lung, Colorectal
and Ovarian (PLCO) cancer screening trial: findings from the initial screen of
a randomized trial. American journal of
obstetrics and gynecology. Nov 2005;193(5):1630-1639.
9. Karen J. Carlson
MSJS, PhD; and Daniel E. Singer, MD. Screening for Ovarian Cancer. Ann Intern Med. 1994;2(121):124-132.
10. Lehtovirta P. Apter D
SU. Serum CA 125 levels during menstrual cycle. Br J Obstet Gynaecol. 1990;10(97):930-933.
11. Tumor markers CA19-9
CA242 and CEA in the diagnosis of pancreatic cancer a meta-analysis. Int J Clin Exp Med. 2015;8(7):11683-11691.
12. Massimo Giona RM,
Antonette E. Leon and Ruggero Dittadi. Comparison of the Diagnostic Accuracy of
CA27.29 and CA15.3 in Primary Breast Cancer. Clinical Chemistry
1999;45(5):630-637.
13. Shimada H, Noie T,
Ohashi M, Oba K, Takahashi Y. Clinical significance of serum tumor markers for
gastric cancer: a systematic review of literature by the Task Force of the
Japanese Gastric Cancer Association. Gastric
cancer : official journal of the International Gastric Cancer Association and
the Japanese Gastric Cancer Association. Jan 2014;17(1):26-33.
14. Michael K. Brawer M.
Prostate Specific Antigen Current Status. CA
Cancer J Clin. 1999;5(49):264-281.
15. Association AU.
Prostate Specific Antigen (PSA) Best Practice Policy Oncology. 2000;14(2):267-286.
16. Carter HB PJ, Metter
EJ, Brant LJ, Chan DW, Andres R, Fozard JL, Walsh PC. Longitudinal Evaluation
of Prostate-Specific Antigen Levels in Men With and Without Prostate Disease. JAMA. 1992;16(267):2215-2220.
17. JE O. Serum
prostate-specific antigen in a community-based population of healthy men.
Establishment of age-specific reference ranges. JAMA 1993;Vol. 270 ((7)):
860-864.
18. Luboldt H-J,
Schindler JF, Rübben H. Age-Specific Reference Ranges for Prostate-Specific
Antigen as a Marker for Prostate Cancer. EAU-EBU
Update Series. 2007;5(1):38-48.
19. Debruyne EN, Delanghe
JR. Diagnosing and monitoring hepatocellular carcinoma with alpha-fetoprotein:
new aspects and applications. Clinica
chimica acta; international journal of clinical chemistry. Sep
2008;395(1-2):19-26.
20. Di Bisceglie AM HJ.
Elevations in serum alpha-fetoprotein levels in patients with chronic hepatitis
B. Cancer 1989;10(15;64):2117-2120.